各位爸爸媽媽大家好,我是朱子宏醫師。
今天想跟大家分享一個在兒童成長門診中,非常奇妙且具備高度臨床價值的生理現象——Minipuberty。這是一篇刊登在 New England Journal of Medicine (NEJM) 的重量級研究,內容雖然小硬,但對於我們了解小孩的發育極有幫助。
什麼是「迷你青春期」?囡仔兄、囡仔姊的成長第一站
我們通常認為青春期是十幾歲才開始的事,但其實在嬰兒時期,小寶貝的身體會經歷一次短暫的性荷爾蒙分泌高峰。
此即為 “minipuberty”。

性荷爾蒙的分泌衝刺 (Surge)
在出生後的 1 到 3 個月內,小孩的下視丘與腦垂腺會變得活躍。這段時間,血液中的荷爾蒙濃度會短暫升高,甚至接近成年人的數值。雖然這不會讓小朋友真的變成熟,但這段「minipuberty」提供的生理資訊,對遺傳與發育門診來說是無價寶。
為什麼迷你青春期對醫師來說很重要?診斷的黃金窗口
這段時期不只是生理現象,更是我們醫師觀察小孩身體機能的重要工具。
偵測先天性發育問題
透過觀測這段時間的 LH (黃體化濾素) 與 FSH (濾泡刺激素),醫師可以早期發現一些潛藏的疾病,例如卡門氏症候群 (Kallmann syndrome)。如果錯過了這個窗口,可能要等到小孩十幾歲沒發育時,我們才能察覺異常。因此,「迷你青春期」可以說是老天爺留給醫師的一個「診斷後門」。
神秘的 KNDy 神經元與醫學新進展
在這次的研究中,特別提到了位於下視丘的 KNDy 神經元(Kisspeptin, Neurokinin B, Dynorphin),它是控制 GnRH 分泌的靈魂人物。
從嬰兒發育到緩解更年期的「面紅濟炸」
有趣的是,研究 KNDy 神經元不只幫助我們了解小孩,也改進了成人醫學。目前已有藥物(如 fezolinetant、Elinzanetant )透過抑制這些神經元的活性,來改善女性更年期的不適。
In 2023, the FDA approved fezolinetant, the first selective NK3R antagonist, for the treatment of moderate to severe VMS associated with menopause. Additionally, elinzanetant, a dual neurokinin-1 and neurokinin-3 receptor antagonist, has demonstrated promising results. The approval application for elinzanetant was supported by positive findings from the OASIS 1, 2, and 3 Phase III clinical studies.
The dual antagonism of NK-1 and NK-3 receptors enhances its efficacy by alleviating menopause-related sleep disturbances and modulating peripheral vasodilatation. In this regard, elinzanetant represents a promising non-hormonal treatment that targets the underlying causes of VMS through NK-1 and NK-3 receptor pathways. The development of neurokinin B antagonist for VMS treatment exemplifies the impact of advanced pharmacological research on gynecological endocrinology.
當感覺面部發熱、潮紅時,海陸客語形容這叫作:

這類醫學科技的改良,讓許多受潮紅與失眠困擾的長輩得到了救贖。
朱醫師的溫馨提醒

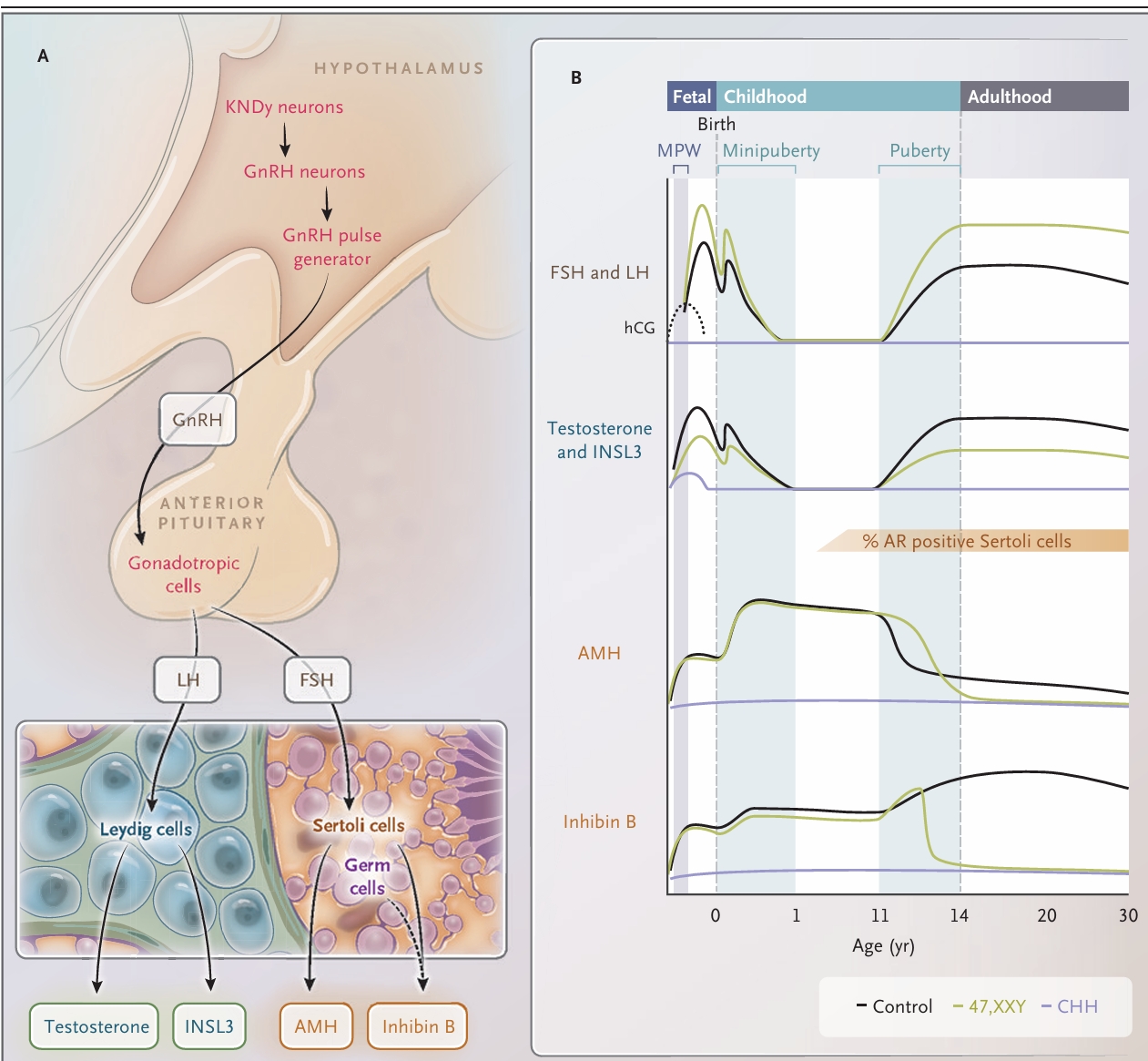
The HPG axis is activated by the integration of neuronal inputs from kisspeptin, neurokinin B, and dynorphin (KNDy) neurons, which stimulate hypothalamic gonadotropin-releasing hormone (GnRH) neurons to induce a pulsatile release of GnRH, which in turn stimulates gonadotropic cells in the anterior lobe of the pituitary gland to secrete follicle-stimulating hormone (FSH) and luteinizing hormone (LH) (Panel A). FSH stimulates Sertoli cells to produce inhibin B and antimüllerian hormone (AMH). Circulating inhibin B consists of
two subunits (α and β); in prepubertal boys, both subunits are derived from Sertoli cells in the testes, whereas in pubertal boys and adult men, the β subunit of inhibin B is derived from germ cells (spermatocytes and round spermatids). LH stimulates Leydig cells to produce testosterone and insulin-like 3 (INSL3). Gonadotropin secretion undergoes three distinct surges: in utero, in early infancy (minipuberty), and during puberty (Panel B). In early pregnancy, placental human chorionic gonadotropin (hCG) stimulates LH receptors on
fetal Leydig cells to produce testosterone in the masculinization programming window (MPW). Patients with congenital hypogonadotropic hypogonadism (CHH) have undetectable FSH and LH at all times, whereas patients with Klinefelter syndrome (the 47,XXY karyotype) have higher gonadotropin levels than controls. Increasing testosterone levels are seen in controls, as well as in patients with congenital hypogonadotropic hypogonadism or the 47,XXY karyotype. After birth, testosterone levels are markedly increased in controls, with peak levels at 1 month of age. At 6 to 12 months of age, testosterone becomes undetectable and remains so until puberty starts. The increase in testosterone and INSL3 levels is reduced in boys with the 47,XXY karyotype, and the levels of testosterone, INSL3, inhibin B, and AMH
remain very low at all ages in patients with congenital hypogonadotropic hypogonadism. Androgen receptor (AR) expression in Sertoli cells begins to increase gradually at 4 years of age, and after puberty 100% of Sertoli cells express AR.
醫學知識日新月異,我們不斷引進國外文獻,就是為了提供給小朋友更好的醫療品質。
如果您發現家中的小孩在成長發育上有任何讓您擔心的地方,歡迎來到診間與我討論。我們一起透過這些精密的科學數據,守護囡仔兄、囡仔姊的健康長大!
參考文獻: Juul A, et al. Clinical Implications of Minipuberty. N Engl J Med 2026;394:1204-14.
Minipuberty refers to a specific period in early postnatal life with high activity of
the hypothalamic–pituitary–gonadal (HPG) hormone axis. In infant boys 1 to 3
months of age, high concentrations of follicle-stimulating hormone and luteiniz
ing hormone are released, which results in high levels of gonadal hormones from
testicular Leydig cells (testosterone and insulin-like 3) and Sertoli cells (inhibin B
and antimüllerian hormone).
The HPG axis is also active in infant girls, who have
adult levels of follicle-stimulating hormone and luteinizing hormone during this
period. Immediately after minipuberty, the HPG axis is silenced for approximately
10 years and is reactivated only with the onset of puberty. Thus, minipuberty rep
resents an early window for diagnosing disorders of sexual differentiation and rare
endocrine disorders, such as congenital hypogonadotropic hypogonadism, and may
help guide dosing of therapeutic interventions including gonadotropin therapy. Of
note, minipuberty predicts adult reproductive capacity
發表迴響